Access Menu
Annual General Meeting Notice 2025
Interventional Radiologist | Niagara Health
CAIR WIR Spotlight - Dr. Ethel Rivas Zuleta
CAIR WIR Spotlight - Dr. Rebecca Spouge
CAIR WIR Spotlight - Dr. Elizabeth Dave
CAIR WIR Spotlight - Dr. Aida Ahrari
CAIR WIR Spotlight - Dr. Fiona Anyumba
CAIR WIR Spotlight - Dr. Alda Tam
Call for CAIR Award 2024 Nominations
Combined Interventional/Body Radiologist – Hamilton General Site, ON
Facetime interview: Dr. Nicolette Sinclair with Dr. Nevin De Korompay
 I met Dr. Nevin De Korompay (NDK) 10 years ago, when we were competing to be the Canadian Association of Radiologists (CAR) Board of Directors resident representative. I won’t say who was selected, but I think he is still bitter. We were both funded by the CAR to attend the ACR annual meeting in Washington DC, as we were both soccer players (please see my bio) and from the prairies (NDK is from Winnipeg) so we got along well. Now that we have both ended up in IR, we have stayed in contact and often share cases and pictures of our dogs. Recently, Dr. De Korompay was a part of a group in Kelowna who started performing endovascular therapy for acute ischemic stroke, building a program from the ground up. I was intrigued by this as I thought he was a “body IR’, like me. I also know that “body IRs” performing EVT is a hotly debated topic. In fact, I recall a debate at a previous CAIR (at that time CIRA) meeting on this topic. Of course, Canadians are so polite I think it ended in a draw, but I wanted to touch base with NDK to get some details. – Dr. Nicollette Sinclair
I met Dr. Nevin De Korompay (NDK) 10 years ago, when we were competing to be the Canadian Association of Radiologists (CAR) Board of Directors resident representative. I won’t say who was selected, but I think he is still bitter. We were both funded by the CAR to attend the ACR annual meeting in Washington DC, as we were both soccer players (please see my bio) and from the prairies (NDK is from Winnipeg) so we got along well. Now that we have both ended up in IR, we have stayed in contact and often share cases and pictures of our dogs. Recently, Dr. De Korompay was a part of a group in Kelowna who started performing endovascular therapy for acute ischemic stroke, building a program from the ground up. I was intrigued by this as I thought he was a “body IR’, like me. I also know that “body IRs” performing EVT is a hotly debated topic. In fact, I recall a debate at a previous CAIR (at that time CIRA) meeting on this topic. Of course, Canadians are so polite I think it ended in a draw, but I wanted to touch base with NDK to get some details. – Dr. Nicollette Sinclair
NS: Holler Nevin! I hope all is well and you are staying safe in Kelowna. Tell me about your practice and training before EVT came into your life?
NDK: Well, I did my radiology residency in Winnipeg and IR fellowship in Vancouver. I had done a few diagnostic cerebral angiograms during residency, none during fellowship. I started practicing in Kelowna in 2016 and helped develop an evolving “body IR” practice, heavy on the interventional oncology, but also including aortic intervention, vascular malformations, UFEs, PAE, and dialysis work. I should also mention that diagnostic cerebral angiograms were a part of the IR practice at Kelowna General, so that did provide a foundation for EVT.
There are four IRs in our practice of 16 radiologists, we have a private clinic and cover services at Kelowna General Hospital (KGH).
NS: How did EVT become part of your practice? Can you explain your current EVT practice/setup?
NDK: Historically, all acute stroke cases were imaged with CT/CTA at KGH or surrounding hospitals, and then transferred to the lower mainland if they were EVT candidates. Transferring these patients obviously takes time, and as you may have heard once or twice, time is brain. Transfer was often prolonged in the winter with unsafe travel conditions. Anecdotally, it was rare for a patient to get to Vancouver in time to still be considered for EVT, or have any quality outcome. KGH is a tertiary referral center for the Okanagan with 441 beds. It is a UBC teaching hospital and distributed site for the Faculty of Medicine.
About 3 years ago, we were going about our “body IR” business when neurology and administration approached us with a request to develop an EVT program, based on success in centers like Kingston and Victoria and their inability to get local patients the gold standard of care. The stroke neurologists were putting together a multidisciplinary stroke team to improve outcomes in the KGH; a team now incorporating neurologists, patient coordinators, nurse navigators, and soon to be IRs and an endovascular neurosurgeon.

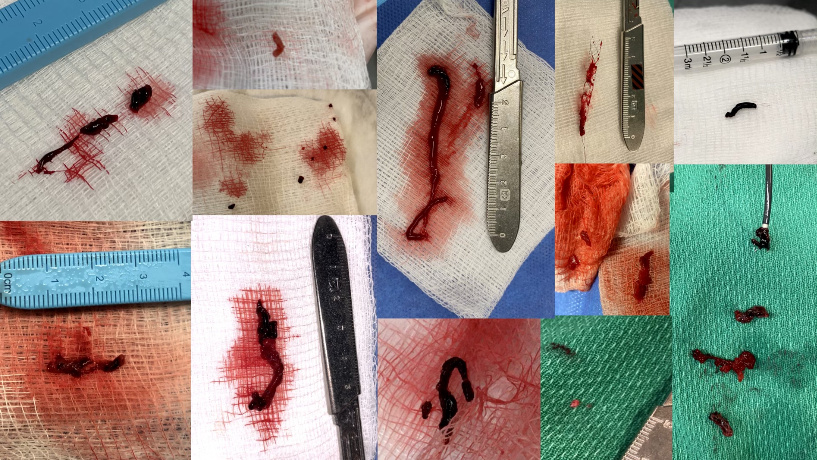
Currently we have 5 EVT operators, 4 IRs and 1 endovascular neurosurgeon, it’s a great group and I would like to mention them by name: Dr. Brooke Cairns, Dr. Paul Kurkjian, Dr. Wayne Tonogai and myself from IR and Dr. Mike Tso from neurosurgery. All cases are reviewed in a group; even after hours whoever is available checks images and weighs in. All cases are performed with two operators scrubbed in, the primary operator is on call, and the second operator is whoever else is available and sober. Sometimes there will be three or four of us there. We did our first EVT case in 2019; we have done over 50 so far. Recently we have undertaken a radial program, mostly to avoid angering Dr. Darren Klass.
We participate in weekly stroke rounds and monthly multidisciplinary conferences with the Victoria group, sharing cases, techniques and outcomes. There are monthly quality meetings involving representatives from radiology, neurology, surgery, anesthesia, nursing, technologists, and even EMTs. Metrics and outcomes are continuously tracked and reviewed. This has unequivocally been a team based approach and we would simply not be able to offer this service without support from a multitude of partners and an exhaustive amount of infrastructure developed behind the scenes. It’s a lot of work but its rewarding work.
NS: What kind of extra training did you do?
NDK: We had proctors from all over Canada come to Kelowna for benchtop device demonstrations and mentoring, we visited other EVT sites, and we were extremely fortunate to have had mentorship from other sites in British Columbia where body IRs provide acute stroke intervention, including New Westminster and Victoria. Then we had to start. Out of the gate we were very selective with cases and rolled out the program during specific, set hours, eventually expanding it to 24/7.
NS: Have you been criticized for being a body IR doing neuro IR? How do you respond to that?
NDK: Probably. Directly to my face, not so much…although meetings have been less frequent in the pandemic. Early on there was always concern in the back of our minds we would do something silly, be deservedly lambasted, and would put patients or the future of the program at risk. That fear has not entirely vanished. Having now participated in these cases, I respect the concerns raised by our neuro IR colleagues for maintaining quality in patient care. I’ve also come to accept that wherever people are asymmetrically distributed, i.e. the world, there will be debate about equal access to procedures, resources, and subspecialists. My opinion is that the right practitioner with the right team in the right environment should be capable of choosing and executing the right cases. The ESCAPE trial, for instance, featured Canadian body IR’s performing EVT and that study represents one of the definitive trials in stroke. Currently, EVT is performed in Canada by Neuro IR, Body IR, Neurosurgery and Interventional neurology depending where you are and on what day. All of our practices are anecdotal in some way, each a unique culmination of geography, patient population, local expertise, referring clinicians, interest, and personalities. We simply would have never have dreamed of starting an EVT program without a demonstrated need, a mandate from our clinicians and a robust multidisciplinary team. I will admit though, I have certainly enjoyed the challenge of working with an amazing team to develop a program I’m proud of and one I wouldn’t hesitate to offer to you if a clot from your frostbitten toes should strike you down via a previously undiagnosed PFO while skiing up at Big White.
NS: Thank you, I will take you up on that offer, please tell everyone I was skiing expertly down a double black at the time. So, do you have any advice for a body IR being asked to provide acute stroke intervention/setting up a practice?
NDK: At risk of sounding like a broken record, you need a team established first before even thinking about sticking needles into anyone. It was their motivation and mandate that got everyone to the table and ultimately resulted in this team being built and we continue to lean heavily on their infrastructure and expertise.
Locally, Getting comfortable with cerebral angios and external carotid work, i.e. crossing the neck barrier, makes it easier to psychologically approach intracranial work which is an intimidating prospect.
I would also recommend reaching out to other sites with body IRs performing acute stroke intervention to learn from their experience as well as to your partners in industry who are happy to facilitate developing expertise in using products with neuro pricing. And speaking of equipment you will need some sort of super nurse or super tech to handle your inventory and ensure all members of the team are comfortable with flushes, triaxial systems, 014 wires, etc. that may not be part of your routine practice.
Finally be ready for lots of meetings. During the work day.
NS: Thank you so much for taking the time to talk to me, congratulations to you and your team for the fine work in Kelowna. Final question, would you attend a CAIR meeting in Saskatoon?
NDK: Little known fact about me, I was actually born in Saskatoon. #BunnyHug
NS: Oh that explains a lot about you!
NDK: But you can’t really expect the first post pandemic in person CAIR meeting to be in Saskatoon? Might I suggest Kelowna?
NS: Fair point, how about the third post pandemic in person CAIR meeting in Saskatoon?
NDK: Yeah, I’ll be there 🙂
Recently, Dr. De Korompay was a part of a group in Kelowna who started performing endovascular therapy for acute ischemic stroke, building a program from the ground up.
An opening for a 2-year fellowship in Vascular & Interventional Radiology at the University of Toronto 2021-2023 has become available.
The Canadian Association for Interventional Radiology (CAIR) condemns the escalating violence and ongoing harassment directed at Asians and Asian Canadians and stands in solidarity and compassion with the diverse Asian community.
Are you passionate about IR and would like to influence positive change? Do you have a solid base of expertise and experience? Do you have fresh ideas and new perspectives?
Woman. Interventional radiologist. You rarely heard those terms together in Manitoba until Dr. Alessandra Cassano-Bailey entered the field of interventional radiology in 2012.
The Department of Radiology at Victoria, British Columbia seeks to recruit a full time Radiologist with Interventional Radiology sub-speciality.
Kamloops Medical Imaging is seeking a locum Interventional Radiologist
With a growing demand for minimally invasive procedures and a large underserved population worldwide, global outreach in IR is growing at a rapid pace. Tanzania is at the center of these advances with road2IR, the first IR training program in Subsaharan Africa. In Tanzania, a country of over 60 million people, there is only 1 diagnostic radiologist per 1 million people and no prior IR service.
CAIR supports interventional radiologists in taking an active role in patient care, including outpatient clinics and inpatient admissions in the care of patients undergoing IR procedures.
Les imprévus vont de pair avec la médecine, un domaine dans lequel la certitude n'existe pas.
 With a growing demand for minimally invasive procedures and a large underserved population worldwide, global outreach in IR is growing at a rapid pace. Tanzania is at the center of these advances with road2IR, the first IR training program in Subsaharan Africa. In Tanzania, a country of over 60 million people, there is only 1 diagnostic radiologist per 1 million people and no prior IR service.
With a growing demand for minimally invasive procedures and a large underserved population worldwide, global outreach in IR is growing at a rapid pace. Tanzania is at the center of these advances with road2IR, the first IR training program in Subsaharan Africa. In Tanzania, a country of over 60 million people, there is only 1 diagnostic radiologist per 1 million people and no prior IR service.





