This segment will feature a unique pearl learned by a junior VIR staff during residency or fellowship to share with our community. This first pearl is written by Dr. Joel Woodley-Cook from Scarborough Health Network.
The Woggle Technique for Obtaining Hemostasis at Hemodialysis Access Sites
The Woggle technique (Simons, Rajan, and Clark 2003) was taught to me by Dr. Martin E. Simons and Dr. Dheeraj K. Rajan at the Toronto Western Hospital late in PGY-5. This “MacGyver” type of method is very handy for achieving hemostasis in any superficial access (I have also used it when accessing superficial dacron arterial bypass grafts) but was initially described for use at hemodialysis (HD) access sites.
The Woggle technique utilizes a superficial purse string suture around the sheath entry site with its ends threaded through the cut tip of the sheath’s dilator, which serves as a tension collar. The sutures are then fed through a stop cock valve (or similar device), which provides the tightening and locking mechanisms for the system. This technique can be used in accesses with or without a skin nick.
The Woggle technique, if performed correctly, obviates the need to obtain manual hemostasis, which can be particularly helpful in patients on anticoagulation or who receive heparin during the procedure. This technique can also help prevent every fellow’s and junior staff’s nightmare scenario of thrombosing a circuit with aggressive manual compression.
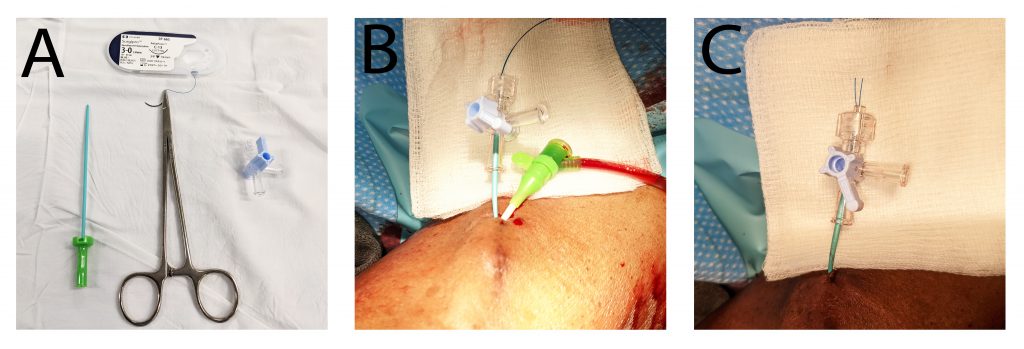
Materials (Figure 1A):
- One suture. I use a 2-0 or 3-0 monofilament suture with a curved cutting needle.
- One sheath dilator tip, cut to approximately 3 cm (these can fly away while cutting, so I (or my assistant) to cut it under a sterile towel). A guide wire introducer can also be used.
- One stop cock (or equivalent).
Method (Figure 1B and 1C):
- Make a superficial purse string suture around the sheath. Be careful not to suture the sheath and/or access vessel. I will sometimes instill lidocaine to create a buffer if the vessel is immediately subdermal.
- Cut the needle off the suture and feed the two free ends through the tapered tip of the cut sheath dilator. Cut the suture flush, leaving around 10 – 15 cm of suture length.
- Once the free suture ends are fed through the dilator tip, feed the suture ends through the stopcock.
- Tell your assistant to stand out of the line of fire (blood squirting) and remove the sheath while tightening the sture by turning the stopcock dial. One-half turn will usually suffice, as the suture may fracture with aggressive turning.
- Leave in situ for 20 – 120 (our patients recover for two hours, so I write orders to D/C the Woggle just prior to discharge, as this length of time reduces risk of bleeding if the patient is anticoagulated).
- When D/Cing the Woggle, turn the dial in the opposite direction used for locking and carefully loosen the device by retracting the dilator tip (stiffening collar). If there is still evidence of arterial bleeding, one can re-initiate the tightening and locking mechanism. If there is no evidence of arterial bleeding, the suture may be removed. Soft manual compression may be required for a brief moment due to mild oozing from the suture removal.
Note: If someone else is disassembling the Woggle, education is important, so be sure they know how it works, why it works, and how to properly disassemble and assemble as required.
Figure: The Woggle. Equipment (A); Woggle created with sheath in situ (B); Woggle in action (C).
Reference:
Simons, Martin E., Dheeraj K. Rajan, and Timothy W. I. Clark. 2003. “The Woggle Technique for Suture Closure of Hemodialysis Access Catheterization Sites.” Journal of Vascular and Interventional Radiology: JVIR 14 (4): 485–88.